For clinicians considering structured platelet-rich plasma (PRP) training, understanding what actually happens before, during, and after a course can make the difference between arriving prepared and leaving confident, versus feeling overwhelmed and unsure. This guide walks through what a quality hands-on musculoskeletal PRP program looks like in practice, from the materials you receive on enrollment to the format options available and the way the day is structured around real patients. By the end, you will have a realistic picture of what a rigorous program delivers and how to prepare to get the most from your training investment.
TLDR: A hands-on musculoskeletal PRP training course at RMA typically runs one full day, with longer multi-day formats in development and custom programs available. The day starts early in the morning, and you begin with hands-on training on real patients rather than sitting through a separate lecture day. The science and regulatory content is woven around the clinical work. Books, ebooks, and other foundational resources are sent to you when you enroll, so you arrive prepared. Three formats are offered: small group at our host facility, private one-on-one at the instructor’s practice, or on-site at your own clinic with your patients and staff. A single course is a starting point, not a credential.
Important Disclaimer
Regenerative Medicine Academy (RMA) is an education company providing training for licensed clinicians. This article is educational content and does not constitute medical advice, legal counsel, or any guarantee of clinical outcomes. Techniques discussed may involve off-label use of FDA-cleared devices and are subject to state and federal regulations. Clinicians are responsible for understanding FDA regulatory status, scope of practice, informed consent, and malpractice implications before implementing any technique. Individual clinical judgment and patient-specific factors must guide all clinical decisions.
You have probably been hearing about PRP from several directions at once. A colleague two offices over mentions offering it for knee pain. A device representative leaves brochures on your desk. A patient with chronic tennis elbow asks whether you do PRP because she saw a professional athlete talk about it online. Somewhere in the middle of all that, you start wondering whether PRP fits in your practice and what it would actually take to learn how to do it well.
The step from reading about PRP to performing it safely is larger than most clinicians realize. Knowing the biology is not the same as knowing how to draw blood correctly, process a sample on a specific centrifuge system, select the right patients, and inject under ultrasound guidance without hitting a nerve or misplacing the injectate. A bad PRP practice creates regulatory exposure, malpractice risk, and patient dissatisfaction. A good one is a legitimate, evidence-informed addition to musculoskeletal care. This guide gives you an honest, structured look at what a quality hands-on PRP training course actually delivers, so you can evaluate programs on substance rather than marketing.
Why formal PRP training matters now
PRP has moved from the margins of musculoskeletal medicine into mainstream clinical conversation. Patients increasingly arrive asking about it by name, and clinicians who want to offer PRP face a choice: learn the procedure through informal exposure and device-rep demonstrations, or complete structured training that covers the science, regulatory framing, evidence, and technique together.
The informal path carries real risk. Clinicians who begin performing PRP without formal training commonly misunderstand the FDA regulatory status, use imprecise language in patient-facing materials, underestimate the importance of ultrasound guidance, and lack a documentation framework that would withstand scrutiny if a patient has a poor outcome. Device representatives can explain their specific preparation system, but they are not a substitute for training that covers patient selection, evidence interpretation, and informed consent. The December 2025 launch of the American Academy of Orthopedic Surgeons (AAOS) Orthobiologics Registry reflects growing institutional recognition that the field needs better-trained clinicians producing better-documented outcomes.
What this means in practice: Formal training is not just about learning a technique. It is about acquiring enough biology, regulatory knowledge, and clinical judgment to use PRP responsibly, communicate honestly with patients, and document defensibly. A well-designed course front-loads that foundation so the hands-on skills you learn are anchored in the right clinical context.
Who MSK PRP training is designed for
Quality MSK PRP training courses are designed for licensed clinicians who already understand injection-based procedures and want to add PRP to their procedural skill set within an evidence-based framework. The typical audience includes physicians (MD/DO) across primary care, sports medicine, orthopedics, physical medicine and rehabilitation, and pain management, along with physician assistants, nurse practitioners, chiropractors, podiatrists, physical therapists, and registered nurses pursuing advanced procedural skills. Eligibility depends on your state scope of practice, which you should verify before enrolling.
MSK PRP courses differ meaningfully from aesthetic PRP courses. Aesthetic training focuses on facial anatomy, scalp injection for hair restoration, and topical PRP applications, with safety concerns centered on vascular occlusion, asymmetry, and superficial nerve injury. MSK training focuses on joint, tendon, and ligament anatomy, with safety concerns centered on septic arthritis (joint infection), nerve and vessel proximity, and correct intra-articular placement. Proficiency in one application area does not transfer to the other.
Introductory courses are suitable for clinicians new to PRP who want foundational knowledge and beginner-level hands-on practice. Advanced courses build on prior injection experience and cover more complex indications, deeper evidence review, and more intensive ultrasound guidance. Most clinicians benefit from completing an introductory MSK PRP training course before considering advanced programming, regardless of existing injection experience.
What you receive when you enroll
When you enroll in an RMA course, the foundational reading materials are sent to you before you arrive. This includes books, ebooks, and curated resources covering PRP biology, the FDA regulatory landscape, and the current evidence base. Reviewing these in the weeks before training is part of why our hands-on day can stay focused on hands-on work. You arrive with the conceptual foundation already in place, and the live time goes toward the parts of training that cannot be delivered through reading: tactile experience, real-time feedback, and clinical pattern recognition.
The materials also stay with you after the course. Many clinicians find themselves referring back to the regulatory section months later when drafting consent forms, or pulling out the evidence review when a patient asks a question they want to answer with a citation rather than an impression. The resources are designed for that reuse, not for one-time consumption.
What this means in practice: Your preparation work is structured for you. You do not need to assemble your own pre-course reading list or hunt for the right textbook. The materials arrive with the curriculum already mapped to them, so the time you put in before the course translates directly into more useful time during it.
Choosing the format that fits you
RMA offers training in three primary formats so the structure can match your situation. The format you choose affects the pace of the day, the level of one-on-one attention, and how directly the curriculum maps to your specific practice.
Small group training
Small group training at our host facility brings five or fewer students per instructor together for a day of hands-on learning with real patients. This is the standard format. It works well for clinicians who want to learn alongside peers, observe other learners receive corrections, and share clinical questions in a group setting. The peer learning effect is real, and many attendees say they learned as much from watching their colleagues’ corrections as from receiving their own.
Private training at the instructor’s practice
Private training brings you to the instructor’s clinical practice for the day. You have the full attention of an experienced physician across every patient case, every blood draw, every ultrasound view, and every injection. This format suits clinicians who want intensive focus on specific indications, prefer a more individualized pace, or have schedule constraints that make group dates impractical. Without other learners to share the day with, the curriculum can move at exactly the speed and depth that works for you.
On-site training at your own practice
On-site training brings the instructor to you. You work with your own patients, your own staff, and your own equipment. The instructor walks through the workflow as it will actually happen in your clinic, which removes the translation step that group training in an unfamiliar facility sometimes creates. This format is well-suited to practices that want their whole team trained together, that want the procedural workflow built around their existing systems, or that have specific patient populations they want to focus on.
Custom focus across all formats
Whichever format you choose, the curriculum can be customized around the indications you most want to emphasize. If your practice primarily sees knee osteoarthritis, the day weights toward intra-articular knee technique and the corresponding evidence base. If you treat a high volume of tendinopathy, the focus shifts there. If your interest is in advanced ultrasound guidance for a specific anatomical area, the time can be allocated accordingly. The course is built around your clinical goals rather than around a generic syllabus.
What this means in practice: You can match the format to your situation rather than forcing your situation to match a single format. Clinicians who learn well in groups have a group option. Those who want one-on-one attention have a private option. Practices that want their team trained together have an on-site option. The customization across all three formats means the day works for your practice rather than for an idealized average attendee.
A typical training day at RMA: hands-on first thing in the morning
Most musculoskeletal PRP training courses at RMA run one full day. Longer multi-day formats are in development for clinicians who want broader exposure or deeper coverage of specific indications. Whether your course is a single day or longer, the structure is the same: the day starts early, and you begin with hands-on training on real patients first thing in the morning.
This sequencing is deliberate. Procedural skill is what most clinicians come to a hands-on course to develop, and procedural skill grows only with supervised hands-on time. Sitting through a half-day of lecture before touching a needle delays that learning. The science and regulatory content is woven around the clinical work instead of stacked in front of it. You discuss the FDA framework while reviewing a real consent conversation. You talk through the evidence base while you are about to inject the joint that the evidence describes. The two reinforce each other.
Early morning: real patients on the schedule
The day usually starts before most clinics are even open. By the time you arrive, real patients are already on the schedule. The instructor walks the small group through the morning’s first case, reviews the imaging and history, demonstrates the consent conversation as he or she would have it, and performs the first procedure. This first observation sets the model for what supervised practice should look like. You see the entire workflow from consent through injection through documentation in a single sequence, on a real patient, in a real clinical setting.
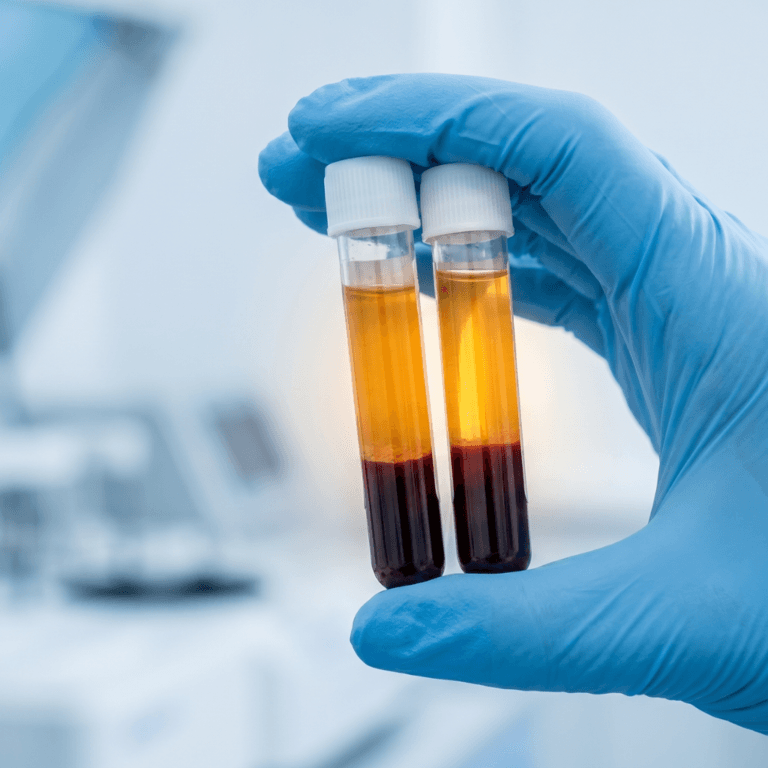
Blood draw and centrifuge processing
Supervised venipuncture follows next, because consistent PRP preparation starts with consistent blood collection. The choice of anticoagulant tube and the draw technique both affect platelet yield, so proficient blood collection is the foundation of the entire procedure. Even clinicians who draw blood routinely often find that supervised practice surfaces small habits worth refining.
You then learn to operate the course’s PRP processing system, including loading the centrifuge, running the separation cycle, and extracting the platelet-rich fraction. The goal is not to memorize a single recipe but to understand the variables in the preparation process and how to apply the manufacturer instructions for use (IFUs) for the specific device you will use in your own practice. Different systems produce different products, and competency on one system does not automatically transfer to another. Watching the visible layering after centrifugation gives a tactile understanding of PRP preparation that no textbook or video replicates.
Ultrasound fundamentals tied to live patient cases
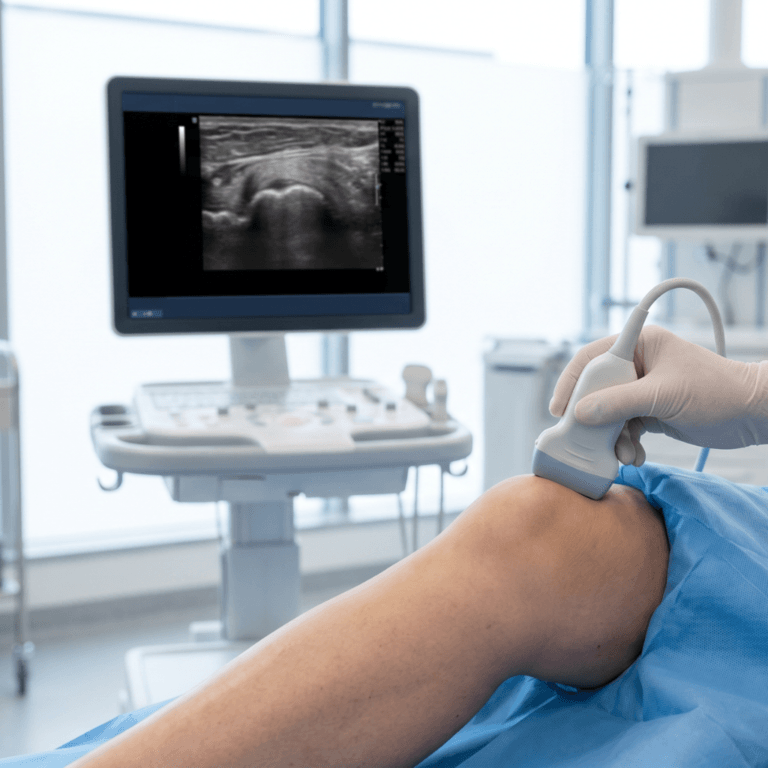
Ultrasound guidance is emphasized in MSK PRP training in a way that distinguishes it from aesthetic PRP courses. Joint and tendon injections carry different anatomical risks than facial injections, and real-time imaging confirmation that the injectate is entering the intended anatomical space is one of the most important safety layers in the procedure.
The ultrasound session typically opens with probe handling, machine setup, gain adjustment, depth settings, and orientation conventions. Attendees practice identifying standard anatomical landmarks: joint spaces, tendon structures, bursal spaces, and the neurovascular structures (nerves and blood vessels) that must be avoided. For most clinicians new to MSK ultrasound, simply learning to find and hold an image of the knee joint or the lateral epicondyle is a meaningful accomplishment in a single day. Needle visualization is then introduced. In-plane technique, where the needle is held parallel to the long axis of the probe so the entire shaft is visible during insertion, is generally preferred for MSK PRP applications because it allows continuous confirmation of needle position.
The realistic goal in an introductory course is orientation and awareness, not mastery. Ultrasound competency develops over many supervised sessions. Good instructors explicitly teach attendees how to recognize when their imaging is not yet confident enough to proceed and what supervision they should seek in early independent cases.
What this means in practice: Ultrasound guidance is not optional decoration in MSK PRP practice. A training program that skips or minimizes this component skips a meaningful safety layer, regardless of how good the rest of the curriculum is.
Supervised injection practice on real patients
Supervised injection practice on real patients is the centerpiece of the day. This is where the small group ratio matters most. With five or fewer students per instructor, every attendee receives direct, individualized feedback on grip, needle angle, aspiration technique, and injection confirmation. Larger groups cannot deliver the same quality of correction, even when the faculty is excellent.
Common injection targets practiced in MSK PRP courses include the knee joint (intra-articular), the lateral epicondyle region for tennis elbow, the plantar fascia origin for plantar fasciitis, and the supraspinatus tendon region for rotator cuff tendinopathy. Practice typically begins with anatomical surface landmark technique and progresses to ultrasound-guided approach, with instructors providing real-time correction. Live patient sessions provide tactile and clinical feedback that simulations cannot reproduce: skin tension, tissue resistance, real-time patient response, and live imaging interpretation under clinical conditions.
Most courses use a “see one, do one, teach one” structure within the small group, with instructor demonstrations followed by supervised attempts followed by peer teaching. Attendees who observe their peers receive corrections learn from those corrections too, which multiplies the effective learning without requiring each clinician to make every mistake personally.
Debrief, documentation, and follow-up planning
The final block of the day covers what happens after the injection ends. Quality programs include explicit instruction on documentation requirements: what to record in the procedure note, how to capture the informed consent conversation, how to log PRP preparation parameters, and what follow-up schedule supports outcome tracking.
Outcome measurement tools introduced in training typically include the Visual Analog Scale (VAS, a 0 to 10 pain severity rating), the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC, which measures pain, stiffness, and function in osteoarthritis patients), and condition-specific scales such as the Patient-Rated Tennis Elbow Evaluation. Follow-up intervals discussed usually include assessments at 6 and 12 weeks, with longer follow-ups at 6 and 12 months to capture the delayed-onset benefit pattern seen in the literature. Clinicians who track outcomes systematically from their first case forward build a personal evidence base that supports better patient selection, improved technique, and honest practice marketing.
The science and regulatory content woven through the day
The didactic content is taught in shorter blocks that connect directly to what you are doing in the clinical workflow. This integrated structure makes the science easier to retain because it lands while your hands and eyes are still on the relevant clinical context.
PRP biology and why preparation variables matter
PRP is an autologous blood product, meaning it comes from the patient’s own blood. A sample is drawn, processed through a centrifuge to concentrate platelets above baseline whole blood levels, and injected into the target tissue. When platelets activate, they release over 300 bioactive proteins, including platelet-derived growth factor (PDGF), transforming growth factor-beta (TGF-beta), vascular endothelial growth factor (VEGF), epidermal growth factor (EGF), and fibroblast growth factor (FGF). Insulin-like growth factor-1 (IGF-1) is also present, primarily from the plasma fraction rather than from platelet alpha granule release. These factors recruit repair cells, support new blood vessel formation, and shape the local inflammation response rather than just suppressing it.
A critical classification distinction is taught early. Leukocyte-poor PRP (LP-PRP) minimizes white blood cell content and tends to have anti-inflammatory properties, which may suit intra-articular applications. Leukocyte-rich PRP (LR-PRP) retains higher white blood cell levels and may be better suited for tendon conditions. Neither classification has been definitively validated as predictive of outcomes, but the distinction matters because different preparation systems produce different products. Anticoagulant choice, centrifuge parameters, platelet concentration, and activation method all affect the final product.
FDA regulatory status: what every trained clinician must know
The regulatory module is one of the highest-value parts of a quality course. The language you use with patients, the claims on your practice website, and the informed consent documentation you create all flow from understanding this correctly.
PRP preparation devices reach the market through the FDA’s 510(k) premarket notification pathway. This is a clearance, not an approval. The cleared indication is to produce platelet-rich preparations to be mixed with bone graft materials in orthopedic surgical procedures. Intra-articular injection for osteoarthritis, tendon injection for tendinopathy, and all other musculoskeletal injection applications are therefore off-label.
Off-label use is legal and standard in medicine. Clinicians may use FDA-cleared devices off-label based on their clinical judgment, but patients must be informed of the off-label status, the mixed nature of the evidence, and the fact that outcomes vary. Quality training programs teach the exact language to use in this conversation and provide documentation frameworks to record that it took place. The language matters: a trained clinician never describes PRP injections as “FDA-approved” for musculoskeletal indications. The accurate framing is “FDA-cleared device used off-label for this application.”
Evidence review: what the literature actually supports
Quality MSK PRP courses review the evidence by condition, not as a marketing pitch but as a framework for clinical decision-making. The strongest evidence supports PRP for mild-to-moderate knee osteoarthritis, lateral epicondylitis, and plantar fasciitis. Across these conditions, the most consistent pattern in recent meta-analyses is a crossover effect: corticosteroids tend to outperform PRP in the first 4 to 6 weeks, while PRP shows more durable benefit at 6 months and beyond. Evidence is weaker or more conflicting for Achilles tendinopathy, rotator cuff repair augmentation, and anterior cruciate ligament reconstruction.
Professional society disagreements are part of the curriculum. The 2024 ESSKA-ORBIT consensus on PRP for knee osteoarthritis issued a Grade A recommendation supporting PRP for mild-to-moderate knee osteoarthritis in three of its 28 statements. The 2019 American College of Rheumatology and Arthritis Foundation guideline strongly recommends against PRP for both knee and hip osteoarthritis. The 2021 Bennell RESTORE trial in JAMA found that PRP was no better than saline at 12 months for pain or cartilage volume in knee osteoarthritis. These contradictions are not a sign that the field is broken. They reflect real heterogeneity in preparation methods, patient populations, outcome measures, and follow-up durations across studies.
What this means in practice: The ability to walk into a patient consultation and accurately describe both the supportive and the conflicting evidence is what separates a clinician who has been trained from one who has only been sold a device. Patients trust honesty more than enthusiasm.
Patient selection, contraindications, and informed consent
Patient selection follows from the evidence base. For knee osteoarthritis, candidates are typically Kellgren-Lawrence (KL) grades I through III who have not responded adequately to conservative care, including physical therapy, weight management, and oral anti-inflammatories. Patients with KL grade IV disease show diminished response in most studies, though the ESSKA consensus allows for carefully selected non-surgical candidates. For tendinopathies, appropriate candidates are typically those with chronic presentations that have resisted conservative management.
Absolute contraindications include active bacterial infection requiring antibiotic therapy, unstabilized hematologic malignancy, active solid cancer undergoing diagnosis or treatment, local infection at the injection site, and recent dental infection or invasive oral procedure. Relative contraindications include thrombocytopenia (low platelet count) below 50,000 per cubic millimeter, NSAID use within the 48 hours before the procedure, and corticosteroid injection at the treatment site within the prior month.
Informed consent is treated as a clinical competency rather than a legal formality. Quality programs provide sample consent forms and walk attendees through the elements that must be discussed: off-label status, evidence quality, realistic response rates (roughly 30 to 40 percent of patients in knee osteoarthritis cohorts do not achieve meaningful improvement), common adverse events, and alternatives to PRP. The conversation itself, documented as a narrative in the chart, is what protects the clinician if a patient later has questions or a poor outcome.
Why instructor-to-student ratios matter
The instructor-to-student ratio in a hands-on clinical training course is one of the most reliable predictors of how much procedural learning actually happens. It is also one of the easiest quality markers to verify before enrolling.
Large lecture-style courses may deliver excellent didactic content, but procedural competency requires direct observation and real-time correction of technique. A 20-to-1 student-to-instructor ratio means most attendees will practice minimally under real supervision, which defeats the point of a hands-on course. Programs that maintain five or fewer students per instructor allow individual feedback on grip, needle angle, aspiration, ultrasound probe position, and patient communication. Small groups also produce a multiplicative learning effect, because attendees learn not just from corrections on their own performance but from watching their peers receive corrections on theirs.
What this means in practice: Before enrolling in any hands-on PRP course, ask the specific question: what is the maximum student-to-instructor ratio during hands-on injection practice? If the answer is vague or the ratio is above 6-to-1 for injection practice, the program is unlikely to deliver the supervised experience that hands-on training should provide.
Hands-on versus online-only training: what each can and cannot teach
Online PRP training has grown quickly in the past few years, and it has a legitimate role. Understanding what online training can and cannot deliver helps you structure your overall learning plan intelligently rather than assuming one format replaces the other.
Online courses effectively deliver the science of PRP, the FDA regulatory framework, the evidence by condition, patient selection criteria, contraindication frameworks, and informed consent principles. These topics are well-suited to self-paced study, can be revisited as often as needed, and carry no logistical barriers. RMA’s online regenerative medicine education covers this foundation for clinicians who want to study at their own pace before adding hands-on training.
What online training cannot deliver is the tactile and real-time experience of performing the procedure. You cannot learn the feel of tissue resistance during injection, the real-time interpretation of an ultrasound image under patient motion, or the kinesthetic memory of a controlled blood draw from a video. You also cannot receive real-time correction from an instructor watching your hand. A clinician who completes only online PRP training has acquired the knowledge to describe PRP but not the supervised experience to perform it safely and reproducibly.
The most efficient learning path is usually a hybrid format: online didactic preparation followed by in-person hands-on practice. This structure lets the classroom time focus on what it does best, supervised skill development, rather than re-covering material that reads well on a screen.
How MSK PRP training differs from aesthetic PRP training
Musculoskeletal PRP training and aesthetic PRP training overlap in their underlying biology but diverge substantially in anatomy, injection targets, safety considerations, ultrasound emphasis, and evidence base. A clinician proficient in one is not automatically proficient in the other.
Aesthetic courses focus on facial anatomy, scalp injection technique for androgenic alopecia (a common cause of pattern hair loss), microneedling protocols, and topical PRP applications. Primary safety concerns center on vascular occlusion, asymmetry of cosmetic outcome, and injury to superficial nerves of the face. MSK courses focus on joint capsules, tendon insertions, ligament anatomy, and the neurovascular structures adjacent to them, with primary safety concerns centered on septic arthritis, proximity to named nerves and vessels, and correct placement within an intended anatomical space. Ultrasound guidance is heavily emphasized in MSK courses because confirming correct needle placement in a joint or peritendinous space is a different skill than avoiding facial vessels.
| Dimension | MSK PRP training | Aesthetic PRP training |
| Primary anatomy | Joints, tendons, ligaments | Face, scalp, skin |
| Injection targets | Intra-articular, peritendinous | Dermal, perifollicular |
| Ultrasound emphasis | Heavy; central safety component | Light; mainly vascular avoidance |
| Evidence base | Knee OA, tendinopathy, plantar fasciitis | Hair loss, facial rejuvenation |
| Primary safety concerns | Septic arthritis, nerve and vessel proximity | Vascular occlusion, asymmetry, superficial nerve injury |
| Typical format | Hands-on day with live patients | Often shorter; may include device-based procedures |
What this means in practice: If you are building both MSK and aesthetic PRP into your practice, plan two distinct training tracks. The underlying biology overlaps, but the clinical skills, evidence interpretation, and safety considerations are different enough that a single course cannot do both well.
After the course: implementing responsibly
Completing a hands-on PRP training course is a beginning, not a finish line. Procedural skills develop across many supervised cases, and the habits you build in your first year of offering PRP will shape your practice for much longer than that.
Early cases should ideally be performed with an experienced peer available for consultation. If no peer is immediately available in your practice, many clinicians maintain contact with instructors or peers from their training cohort for case discussion. Patient selection in the early months should lean toward straightforward presentations: mild-to-moderate knee osteoarthritis in healthy patients, uncomplicated lateral epicondylitis, and plantar fasciitis without significant comorbidities. Complex cases are better suited to practice that comes after additional supervised experience.
Documentation systems should be in place before the first case. Informed consent language, procedure note templates, outcome tracking forms, and follow-up scheduling should be operational on day one of your new service, not built reactively after problems emerge. Insurance coverage for PRP musculoskeletal injections is generally not available because these uses are off-label, so you need a transparent out-of-pocket pricing structure and financial counseling workflow before offering the service. Malpractice carriers should be notified when you add PRP to your procedures. Most will simply confirm coverage, but the notification creates a paper trail that protects you. Consultation with legal counsel is appropriate if your state has specific requirements for regenerative medicine practices.
What this means in practice: A course graduate who treats the certificate as the end of training is at higher risk of poor outcomes and regulatory problems than one who treats it as the foundation for a structured first year. Responsible implementation is a project, not an event.
A clinical perspective from a fictional first attendee
The following vignette is a fictional composite created for educational purposes. It does not represent a real attendee.
Dr. Rivera is a family medicine physician with three years in practice who has noticed an uptick in patients asking about PRP. She enrolls in an introductory hands-on MSK PRP training course at RMA to evaluate whether to add PRP to her practice.
Two weeks before her course date, a package arrives at her office. It contains the foundational reading materials: books on PRP biology, an ebook on the FDA regulatory framework, and curated articles on the evidence base. She works through them in the evenings over the two weeks, which means she arrives the day of her course with the conceptual material already in her head. She did not have to assemble her own reading list, and the curriculum she is about to walk into is mapped to the materials she just finished.
The morning starts early. By 7 a.m. she is at the host facility, and the first patient of the day is already on the schedule. The instructor reviews the case with the small group, walks through the consent conversation as he would have it, and demonstrates the procedure from setup through documentation. Dr. Rivera realizes she had been about to use the phrase “FDA-cleared for knee injections” in her own intake materials. The course’s regulatory framing clarifies that the devices are cleared only for bone graft handling, and that all injection applications are off-label. She updates her language in a notes app between cases. This is one of the most valuable corrections of the day, and it happens before she touches a needle herself.
Her first supervised blood draw produces adequate volume, but the instructor notes a tourniquet technique refinement she would never have caught from a video. During ultrasound orientation, she is surprised by how different a live knee joint looks under imaging compared to anatomical diagrams. The instructor spends time with her on probe orientation and helps her reliably find the suprapatellar recess. During supervised injection practice on the day’s third patient, she observes two instructor demonstrations before attempting her own, and the real-time feedback on her needle angle is immediate and specific in a way that no written protocol could replicate.
The most important thing Dr. Rivera says she gained from the course is not technique confidence. She knows she needs more supervised cases for that. What she gained is clarity about what she knows and what she still needs to practice. That clarity is where responsible implementation starts.
Frequently asked questions
What license types are eligible for hands-on PRP training?
Most quality programs accept MD/DO, PA, NP, chiropractors, podiatrists, physical therapists, registered nurses, and other licensed clinicians, though eligibility varies by state scope of practice. Verify your state medical board’s position on PRP injections before enrolling and before offering the procedure in practice.
How long does a hands-on MSK PRP training course typically take?
Most RMA musculoskeletal PRP courses run one full day, with longer multi-day formats in development. The day starts early in the morning and is built around hands-on training with real patients. The science and regulatory content is woven through the day rather than delivered as a separate lecture session.
What does RMA send me when I enroll?
When you enroll, the foundational reading materials are sent before the course. This includes books, ebooks, and curated resources covering PRP biology, the FDA regulatory landscape, and the current evidence base. Working through these in the weeks before training is part of why the live day can stay focused on hands-on skills.
Can the training be delivered at my own practice?
Yes. RMA offers on-site training where the instructor comes to your clinic and you work with your own patients, your own staff, and your own equipment. This format suits practices that want their team trained together or that want the workflow built around their existing systems.
Can the curriculum be customized to my practice focus?
Yes. Across all three training formats (small group, private at the instructor’s practice, and on-site at your clinic), the curriculum can be customized around the indications you most want to emphasize. If your practice primarily sees knee osteoarthritis, the day weights toward that. If you treat a high volume of tendinopathy, the focus shifts there.
Do I need prior injection experience to enroll?
Introductory courses are designed for clinicians with basic anatomical knowledge and clinical training, though prior injection experience accelerates learning. Advanced courses typically assume prior experience with corticosteroid or hyaluronic acid injection technique. Working through the pre-course reading materials before arriving is strongly recommended regardless of prior experience.
Is a hands-on PRP course enough to start offering PRP in my practice?
A single hands-on course provides foundational knowledge and introductory procedural experience. Most experienced instructors frame the course as a beginning rather than a completion. Ongoing mentorship, peer case consultation, and systematic outcome tracking are essential components of responsible implementation, and your malpractice carrier should be notified when you add new procedures.
Will I practice on real patients or anatomical models?
RMA courses use real patients for the hands-on portion of the day, starting first thing in the morning. Live patient sessions provide tactile and clinical feedback that simulations cannot reproduce: skin tension, tissue resistance, real-time patient response, and live imaging interpretation under clinical conditions.
How do I know if a PRP training program is high quality?
Key indicators include small group ratios (five or fewer students per instructor during hands-on practice), live patient sessions, faculty with real-world MSK injection experience, explicit coverage of FDA regulatory status and informed consent, honest presentation of evidence (including conflicting findings), and provision of consent forms and documentation templates. Programs that teach technique without regulatory and evidence content leave clinicians exposed.
What should I do if a serious adverse event occurs after a PRP injection?
For suspected serious adverse events involving FDA-regulated medical devices, clinicians may consider reporting through FDA MedWatch consistent with institutional policy. Septic arthritis following any intra-articular injection, though rare, requires prompt recognition, diagnostic aspiration, and appropriate antibiotic treatment. Notify your malpractice carrier of any serious adverse events and document your clinical response thoroughly.
Key takeaways
- Hands-on MSK PRP training at RMA typically runs one full day, with longer multi-day formats in development. The day starts early in the morning with hands-on training on real patients, and the science and regulatory content is woven around the clinical work rather than stacked in front of it.
- RMA sends foundational reading materials, including books, ebooks, and curated resources, to enrolled clinicians before the course, so live time can stay focused on the parts of training that cannot be delivered through reading.
- Three training formats are available: small group at the host facility, private one-on-one at the instructor’s practice, and on-site at your own clinic with your patients and staff. The curriculum can be customized to focus on the indications most relevant to your practice.
- PRP preparation devices are FDA-cleared for bone graft handling only. All injection applications for joints, tendons, and soft tissue are off-label, and quality training programs teach this distinction explicitly alongside informed consent frameworks.
- Small group ratios, typically five or fewer students per instructor during hands-on injection practice, are one of the strongest predictors of procedural learning quality and should be verified before enrolling.
- MSK PRP training differs meaningfully from aesthetic PRP training in anatomy, ultrasound emphasis, safety concerns, and evidence content. Proficiency in one does not transfer to the other.
- A single course is a beginning, not a credential. Responsible implementation requires post-course mentorship, careful early case selection, systematic outcome tracking, and consultation with your malpractice carrier before launching the service.
About Regenerative Medicine Academy
Regenerative Medicine Academy (RMA) is a medical education company providing hands-on, small-group regenerative medicine training courses for licensed healthcare professionals. RMA does not provide clinical treatments or medical services. All course content is educational and designed to support clinicians in making informed, evidence-based decisions within their scope of practice. For information on upcoming training dates, visit regenmedacademy.com.
Off-label use note
Procedures discussed in this article involve off-label use of FDA-cleared devices. Off-label use means the FDA has not specifically approved the device for the described indication. Clinicians may use FDA-cleared devices off-label in their clinical judgment but must obtain informed consent, discuss evidence, risks, and alternatives, and document thoroughly.
Platform and jurisdiction note
Scope of practice, supervision requirements, and corporate practice of medicine rules vary by state. Clinicians should consult their state medical board, malpractice carrier, and legal counsel regarding compliance in their jurisdiction before offering regenerative procedures.
For clinicians ready to take the next step
Clinicians who want to evaluate whether structured training fits their practice can review RMA’s full course catalog, which covers musculoskeletal, cosmetic, sexual health, and adipose tissue applications. The catalog includes group training dates, private training options, and on-site training availability for practices that want their team trained together with their own patients and workflow.