Platelet-rich plasma (PRP) has become one of the most discussed topics in musculoskeletal medicine, yet many clinicians still lack a clear picture of what the evidence actually supports. This guide breaks down the science, regulatory status, condition-by-condition evidence, safety profile, and patient selection criteria so you can make informed decisions about whether PRP fits your clinical practice.
TLDR: PRP devices are FDA-cleared for bone graft handling only; all injection uses for joints, tendons, and soft tissue are off-label. The strongest evidence supports PRP for mild-to-moderate knee osteoarthritis and lateral epicondylitis, with multiple meta-analyses showing modest improvements in pain and function at 6-12 months. However, professional societies disagree on recommendations, and preparation methods vary widely across studies. Read on to understand regulatory nuances, honest evidence gaps, and how to counsel patients ethically.
Important Disclaimer
Regenerative Medicine Academy (RMA) is an education company providing training for licensed clinicians. This article is educational content and does not constitute medical advice, legal counsel, or a guarantee of clinical outcomes. Techniques discussed may be used off-label and are subject to state and federal regulations. Clinicians are responsible for understanding FDA regulatory status, scope of practice, informed consent, and malpractice implications before implementing any technique in practice. Individual clinical judgment and patient-specific factors must guide all clinical decisions.
You have probably heard the pitch before. A device representative calls your office with brochures showing impressive before-and-after data. Your colleagues across the hall started offering PRP injections last year. Patients come in asking for it by name after watching a social media video. But when you dig into the literature, the picture gets complicated fast.
The reality is that PRP occupies a unique space in musculoskeletal medicine. It has genuine biological plausibility, a growing body of meta-analytic evidence, and real clinical adoption. It also has significant preparation variability, conflicting guideline recommendations, and important regulatory distinctions that many clinicians misunderstand. Getting the facts right matters because misinformation in this space can waste patient money, delay effective care, create regulatory exposure, and damage your professional credibility.
This guide walks you through the current state of PRP for musculoskeletal conditions. You will learn what PRP actually is at the molecular level, what the FDA has and has not cleared, what the latest meta-analyses and guidelines say for each condition, and how to select patients and set realistic expectations. By the end, you will have the clarity you need to decide whether PRP belongs in your practice, backed by evidence rather than marketing.
What is PRP and how does it work?
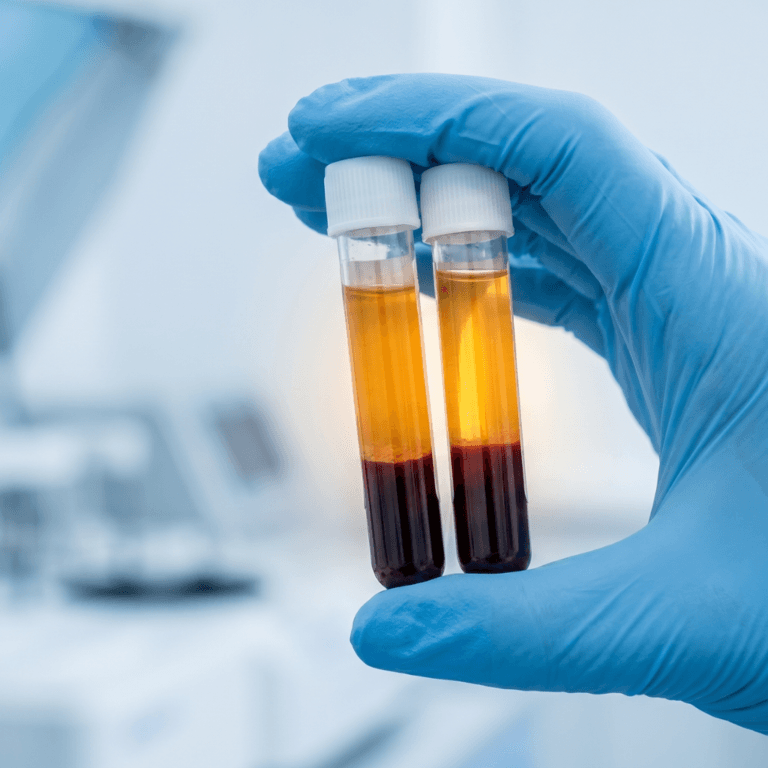
Platelet-rich plasma is an autologous blood product, meaning it comes from the patient’s own blood. A clinician draws a small sample of venous blood and processes it through a centrifuge. The centrifuge separates red blood cells from a concentrated layer of platelets and plasma. The result is a preparation with platelet concentrations typically 5-8 times higher than normal whole blood.
The biological rationale for PRP centers on the concentrated delivery of platelet-derived growth factors. When platelets activate, they release over 300 bioactive proteins that play roles in tissue repair and inflammation regulation. These include platelet-derived growth factor (PDGF), transforming growth factor-beta (TGF-beta), vascular endothelial growth factor (VEGF), and insulin-like growth factor-1 (IGF-1).
These growth factors work through several overlapping pathways. They recruit repair cells to the injury site. They promote new blood vessel formation, a process called angiogenesis. They modulate inflammation by shifting the immune response toward tissue repair rather than tissue breakdown. The fibrin matrix that forms when platelets activate also creates a biological scaffold that traps growth factors and supports cell migration during healing.
The following table summarizes the primary growth factors concentrated in PRP and their roles in tissue repair. PDGF stands for platelet-derived growth factor. TGF-beta stands for transforming growth factor-beta. VEGF stands for vascular endothelial growth factor. EGF stands for epidermal growth factor. IGF-1 stands for insulin-like growth factor-1. FGF stands for fibroblast growth factor. Extracellular matrix (ECM) refers to the structural network of proteins and molecules that surrounds cells in tissues.
| Growth factor | Primary role in tissue repair |
| PDGF | Recruits fibroblasts, stimulates cell growth, promotes ECM production |
| TGF-beta | Drives fibroblast activity, supports blood vessel formation, reduces inflammation |
| VEGF | Promotes new blood vessel growth and supports wound healing |
| EGF | Stimulates growth of fibroblasts, endothelial cells, and skin cells |
| IGF-1 | Promotes cell growth, differentiation, and tissue development (present in PRP primarily via the plasma fraction rather than platelet alpha granule release) |
| FGF | Supports cell growth and tissue repair across multiple tissue types |
What this means in practice: PRP does not work through a single mechanism or “magic bullet.” It influences multiple repair pathways at once through these overlapping growth factors. This helps explain why clinical response varies by tissue type, injury severity, and patient biology. It also explains why standardizing preparation matters for reproducible outcomes.
PRP is more than LP versus LR: leukocyte subtypes and platelet dose
The most common way clinicians categorize PRP is by leukocyte content: leukocyte-poor PRP (LP-PRP) versus leukocyte-rich PRP (LR-PRP). This binary framing is useful as a starting point, but the underlying biology is more nuanced. Two issues are worth understanding in detail: the type of leukocytes actually present in the preparation, and the total platelet dose delivered to the tissue.
The leukocyte question is really about subtypes
White blood cells are not a single category. They include five main types: neutrophils, lymphocytes, monocytes, eosinophils, and basophils. Each plays a different role in immunity and healing.
Centrifugation does not concentrate all five types equally. A 2023 study of 335 knee OA patients (Turajane et al., Cureus) found that PRP preparation actually doubles the lymphocyte ratio compared to whole blood while cutting the neutrophil ratio roughly in half. This means that even “leukocyte-rich” PRP is typically lymphocyte-predominant, not neutrophil-dominant as many clinicians assume.
The clinical concern about leukocytes is mainly about neutrophils. Neutrophils release reactive oxygen species, matrix metalloproteinases, and inflammatory cytokines that can damage cartilage and tendon tissue. Lymphocytes and monocytes appear largely beneficial. Monocytes in particular polarize into M1 and M2 macrophages, which together drive the shift from acute inflammation to tissue repair. Limited peer-reviewed musculoskeletal data exist for eosinophils and basophils, so claims about their healing role remain unproven.
Whole blood normally contains five main types of white blood cells, each with a different role in immunity and healing. Their proportions in whole blood and in PRP differ. The following table summarizes the five leukocyte types and their likely roles based on current evidence. M1 macrophages are pro-inflammatory immune cells. M2 macrophages support tissue repair.
| Leukocyte type | Approximate share in whole blood | Behavior in PRP | Likely role in healing |
| Neutrophils | 50-70% | Often reduced after centrifugation | Pro-inflammatory; may damage cartilage and tendon |
| Lymphocytes | 20-40% | Often increased after centrifugation | Modulate immune response; generally beneficial |
| Monocytes | 2-10% | Variable concentration | Drive M1 to M2 macrophage polarization; key for tissue repair |
| Eosinophils | 1-4% | Limited data | Role in PRP largely unproven |
| Basophils | Less than 1% | Limited data | Role in PRP largely unproven |
For tissue selection, the evidence broadly supports LP-PRP for intra-articular applications like knee OA and rotator cuff repair augmentation. Tendinopathy evidence is more mixed: LR-PRP has shown benefit for lateral epicondylitis, while patellar tendinopathy and chronic Achilles tendinopathy show less consistent results regardless of preparation. Notably, the only direct head-to-head RCT comparing LP-PRP and LR-PRP for knee OA (Di Martino et al., 192 patients) found no significant difference at 12 months on standard outcome measures. This suggests the LP versus LR label may matter less than total platelet dose, neutrophil content, and individual donor biology.
The platelet dose debate
Marketing claims often state that PRP requires 10 billion platelets to be effective. This figure traces back primarily to a single 2021 RCT by Bansal and colleagues, published in Scientific Reports. That study tested one dose level rather than comparing multiple doses head-to-head, so the “10 billion threshold” is an inference from one dose group rather than a finding from a dose-finding trial. Only one to three studies directly support this specific number.
The broader dose-response literature points to a different picture. A 2025 systematic review by Berrigan and colleagues, published in Arthroscopy, analyzed 31 PRP arms across knee OA RCTs. Positive-outcome trials averaged about 5.5 billion platelets per injection, while no-difference trials averaged about 2.3 billion. The authors concluded that doses below roughly 2.5 billion appear ineffective, while doses above 5 billion show consistent clinical benefit.
A 2024 triple-blind RCT by Patel and colleagues, published in Orthopaedic Journal of Sports Medicine, directly compared an 8 mL “superdose” (about 5.65 billion platelets) to a 4 mL conventional dose (about 2.82 billion). The higher dose produced significantly better WOMAC and KOOS scores. The 2021 RESTORE trial, the largest negative knee OA PRP study, used only about 1.6 billion platelets per injection, well below current effectiveness thresholds. Many clinicians now interpret RESTORE’s negative result as evidence of underdosing rather than evidence that PRP does not work.
There is also evidence that more is not always better. A 2026 meta-analysis by Hooper and colleagues, published in PM&R, classified knee OA PRP doses as low (1-5 billion), moderate (5-10 billion), and high (over 10 billion). Moderate doses produced the greatest functional improvement. High doses (over 10 billion) showed less pain reduction at 6 months than the 1-10 billion range. This suggests a possible “sweet spot” in the 5-10 billion range, with diminishing or even slightly negative returns at very high doses. Proposed mechanisms include growth factor receptor saturation, excessive TGF-beta signaling, and prolonged inflammatory activation.
No professional society currently endorses a specific numeric platelet dose minimum. The ESSKA-ORBIT 2024 consensus, AAOS 2024 Technology Overview, and AMSSM 2021 position statement all emphasize careful characterization without naming a threshold. The Biologics Association/Arthroscopy modified Delphi consensus explicitly states that “the ideal dose of PRP is undetermined.”
What this means in practice: The “leukocyte-poor versus leukocyte-rich” distinction and the “10 billion platelet” claim are both directionally useful but quantitatively unproven. The leukocyte concern is really about neutrophils, while monocytes and lymphocytes appear net beneficial. For knee OA, aiming for at least 3 billion platelets per injection appears to be the lower threshold for therapeutic effect, with 5-10 billion representing the strongest evidence-based target. Clinicians should evaluate manufacturer claims based on absolute delivered platelet dose, the leukocyte differential (especially neutrophil content), and whether the system has been used in published RCTs at the same protocol the clinician will use.
Multiple classification systems exist to categorize PRP preparations, including systems based on platelet concentration, leukocyte content, activation method, and red blood cell presence. None of these systems have been validated as predictive of clinical outcomes, and this lack of standardization is one of the biggest challenges in PRP research today.
The transition from laboratory biology to clinical application brings us to a critical regulatory question that every clinician must understand clearly.
FDA regulatory status: what is actually cleared
PRP preparation devices reach the market through the FDA’s 510(k) premarket notification pathway. Under this pathway, manufacturers demonstrate that their device is “substantially equivalent” to a device already on the market. This is a clearance, not an approval, and the distinction is important.
PRP preparation systems, including centrifuge kits, tubes, and separators, are cleared for producing platelet-rich preparations to be mixed with bone graft materials to enhance bone graft handling properties in orthopedic surgical procedures. Recent 510(k) clearances in 2024 confirm this limited indication. For example, OrthoAscent (BK241083), Arthrex Thrombinator System (BK241060), and Healeon Float PRP devices (BK241095) were all cleared for bone graft handling.
What is not FDA-approved: intra-articular injections for osteoarthritis, tendon injections for tendinopathy, intramuscular injections for muscle injuries, or any other non-bone-graft application. All of these uses are considered off-label.
Off-label use is legal and common in medicine. Clinicians may use FDA-cleared devices off-label based on their clinical judgment. However, patients must be informed that the use is off-label, that evidence is mixed, and that outcomes are not guaranteed. Documentation of informed consent is essential.
What this means in practice: If you are offering or considering PRP injections for knee OA, tennis elbow, plantar fasciitis, or any other musculoskeletal condition, you are practicing off-label. This is legally permissible, but it requires transparent communication with patients about the regulatory status. Never describe PRP injections as “FDA-approved” for these indications.
Understanding the regulatory landscape sets the stage for evaluating what the clinical evidence actually shows, condition by condition.
The evidence by condition: what the research says
The PRP evidence base varies significantly across musculoskeletal conditions. Some indications have multiple large meta-analyses supporting clinical benefit. Others have weak or conflicting data. Here is an honest assessment of the current evidence for the most commonly studied conditions.
Knee osteoarthritis: the strongest evidence base
Knee osteoarthritis has the most robust PRP evidence of any musculoskeletal condition, though even here the picture is nuanced.
A 2025 systematic review and meta-analysis published in Cureus included 6 high-quality randomized controlled trials (RCTs) with 1,162 total patients. It concluded that PRP injections may help patients with mild-to-moderate OA. A separate 2025 meta-analysis of 28 RCTs (n=3,246) found that PRP demonstrated comparable pain relief to hyaluronic acid (HA) but superior functional improvement, especially when combined with HA. However, findings are not uniform across meta-analyses. A concurrent 2025 meta-analysis of 15 double-blind RCTs (n=1,632) reported statistically significant and clinically meaningful superiority of PRP over HA for both pain and function at 12 months. The disparity between “comparable” and “superior” findings across these concurrent analyses reflects differences in included studies, preparation methods, and statistical approaches.
Network meta-analyses, which compare multiple interventions simultaneously, consistently show PRP performing better than HA, corticosteroids, and saline on pain and function scores at 6 and 12 months. Benefits appear most robust at 6 or more months, while short-term superiority (3 months or less) is less consistent.
The ESSKA-ORBIT Consensus, published in 2024, issued a Grade A recommendation supporting PRP for mild-to-moderate knee OA, classified as Kellgren-Lawrence (KL) grades I through III on the standard radiographic severity scale. Real-world data from Mayo Clinic, based on over 1,100 treated patients, suggests approximately 60-70% of patients achieve at least 50% improvement in pain and function lasting 6-12 months.
However, not all professional societies agree. The 2019 ACR/AF guideline conditionally recommends against PRP for knee OA and strongly recommends against it for hip OA, citing lack of standardization and heterogeneous evidence. The distinction matters under GRADE methodology: a strong recommendation applies to nearly all patients, while a conditional recommendation is more sensitive to individual values and preferences. The AAOS 2024 Technology Overview makes no recommendation for or against PRP, noting substantial limitations in existing studies. Benefits are most robust in KL grades I through III. Patients with severe OA (KL grade IV) generally show diminished response, though ESSKA guidance notes that PRP may still be considered for carefully selected KL IV patients who are not surgical candidates or who decline surgery.
The following table summarizes how major professional societies have positioned themselves on PRP for musculoskeletal applications. The Kellgren-Lawrence scale is a radiographic grading system for osteoarthritis severity, ranging from grade I (doubtful narrowing) to grade IV (severe joint space narrowing with bone-on-bone changes).
| Society | Year | Position on PRP |
| ESSKA | 2024 | Grade A recommendation for mild-to-moderate knee OA |
| AAOS | 2024 | No recommendation for or against; calls for more research |
| ACR/AF | 2019 | Conditionally recommends against for knee OA; strongly recommends against for hip OA |
| AOSSM | 2024 | Describes PRP as a promising symptom modification option for knee OA (per Sports Medicine Update; not a formal CPG) |
| GRIIP | 2025 | Consensus on contraindications for patients with complex comorbidities |
What this means in practice: If a patient with mild-to-moderate knee OA asks about PRP, you can honestly say that multiple studies show modest improvements in pain and function compared to other injectables, particularly at 6-12 months. But you must also disclose that major societies disagree, the use is off-label, and not every patient responds. Shared decision-making with realistic expectations is the appropriate standard of care.
Lateral epicondylitis: strongest long-term data
Lateral epicondylitis, commonly known as tennis elbow, shows some of the most consistent PRP evidence at long-term follow-up.
A 2026 RCT with one-year follow-up found that corticosteroid injections provided greater short-term improvement at 4 and 8 weeks (p < .001 and p = .003, respectively). At 26 and 52 weeks, PRTEE scores numerically favored PRP (52-week mean: 14.4 versus 29.6), though these differences did not reach statistical significance (p = .07 and p = .10, respectively). The trend consistently favored PRP over the long term. Notably, a secondary outcome measure (QuickDASH) did reach statistical significance at both 26 and 52 weeks (p = .05), supporting durable benefit on at least some functional measures. A 2025 systematic review of 12 studies confirmed this general pattern: corticosteroids work faster, but PRP appears to provide more durable relief.
Current clinical recommendations support LR-PRP specifically for lateral epicondylitis. The 2025 EFORT evidence-based guidelines on orthobiologics found improvements surpassing the minimal clinically important difference (MCID), which is the smallest change that patients perceive as meaningful.
Plantar fasciitis: strong effect sizes
Plantar fasciitis, an inflammation of the thick band of tissue running along the bottom of the foot, has some of the largest effect sizes in the PRP literature.
A 2024 meta-analysis by Herber and colleagues included 21 RCTs with 1,356 patients. PRP showed significant superiority over placebo, corticosteroids, and extracorporeal shockwave therapy (ESWT) for pain reduction. However, no significant differences were observed for reduction of plantar fascia thickness or foot function scores. This suggests that PRP may primarily provide pain relief rather than structural tissue change in this condition.
Rotator cuff tendinopathy: short-term benefits, limited durability
A 2025 systematic review of 30 RCTs with approximately 2,500 participants found PRP significantly reduced pain and improved function in the short term compared to placebo and corticosteroids. However, long-term benefits beyond 12 months were limited, with retear rates and function similar to control groups. A separate 2025 meta-analysis found PRP provided superior functional improvement over corticosteroids at 12 and 24 weeks, though overall pain reduction was similar.
Other conditions: mixed or limited evidence
For hamstring injuries, a 2025 meta-analysis (8 studies, n=330) showed PRP combined with physical therapy produced a shorter return-to-play time compared to physical therapy alone, with a mean difference of about 2.3 fewer days. A 2026 meta-analysis focused specifically on acute hamstring injuries (6 RCTs, n=277) found a larger effect of approximately 8.6 fewer days to return to play, though heterogeneity was very high (I² = 94.1%) and certainty of evidence was rated as low to moderate. The difference in effect sizes across these two analyses reflects different study populations (all hamstring injuries versus acute injuries only) and different inclusion criteria. For elite athletes, even modest reductions in recovery time may be meaningful; for recreational patients, the clinical significance is less clear.
For Achilles tendinopathy, a 2025 umbrella review concluded that PRP may not be effectively changing the underlying disease process in chronic cases. Results for hip OA are growing but lag behind knee OA. For ACL reconstruction augmentation, most RCTs show no consistent functional improvement, though some MRI data suggests improved graft appearance.
Understanding the contradictory evidence
One of the most important things to understand about PRP is that the evidence genuinely conflicts, and this is not simply a matter of “needing more studies.” Respected professional societies have reviewed overlapping bodies of literature and reached different conclusions. The following table summarizes the state of evidence across major conditions.
The visual analog scale (VAS) measures pain intensity on a 0-10 scale. The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) measures pain, stiffness, and function in OA patients. The Patient-Rated Tennis Elbow Evaluation (PRTEE) measures pain and function in lateral epicondylitis. The International Knee Documentation Committee (IKDC) score assesses knee function after ligament injury.
| Condition | Positive findings | Negative or neutral findings |
| Knee OA | Multiple meta-analyses show VAS and WOMAC improvement versus HA, corticosteroids, and placebo at 6-12 months | ACR/AF 2019 conditionally recommends against (knee) and strongly recommends against (hip); AAOS makes no recommendation; high bias across studies |
| Lateral epicondylitis | PRTEE scores numerically favored PRP at 26 and 52 weeks; secondary outcomes (QuickDASH) reached significance | Primary outcome did not reach statistical significance at 26 or 52 weeks; corticosteroids outperform PRP at 4-8 weeks |
| Rotator cuff | Short-term pain relief and functional improvement versus corticosteroids | Long-term benefits beyond 12 months similar to control; retear rates unchanged |
| Achilles tendinopathy | Some positive short-term pain reduction data | Umbrella review found no consistent structural improvement |
| ACL reconstruction | Some MRI evidence of improved graft maturation | No functional outcome improvement in multiple RCTs |
What this means in practice: These contradictions are not a sign that the research is broken. They reflect genuine complexity. Different studies use different PRP preparations (LP-PRP versus LR-PRP with varying platelet concentrations and leukocyte differentials), different platelet doses (often ranging from under 2 billion to over 10 billion per injection), different patient populations (varying OA severity, age, BMI), different outcome measures (VAS versus WOMAC versus condition-specific scales), and different follow-up durations. Industry-funded versus independent studies may also introduce bias. Clinicians should present both sides honestly and engage in shared decision-making with patients rather than cherry-picking only the favorable data.
A clinical perspective on PRP decision-making
The following vignette is a fictional composite created for educational purposes. It does not represent a real patient.
Dr. Martinez is a family medicine physician who recently completed advanced PRP certification training. Her patient, a 54-year-old recreational tennis player, presents with bilateral knee pain that has not responded to physical therapy, weight management, or oral anti-inflammatories over the past 18 months. Imaging shows KL grade II changes bilaterally.
Dr. Martinez reviews the evidence and explains several key points during the consultation. She tells the patient that PRP preparation devices are FDA-cleared for bone graft handling, and that injection for knee OA is considered off-label use. She shares that multiple studies show modest improvement in pain and function at 6-12 months for mild-to-moderate OA, but that a major U.S. guideline (ACR/AF 2019) conditionally recommends against it for knee OA while a European consensus (ESSKA 2024) supports it. She notes that roughly 60-70% of patients in large cohorts report meaningful improvement, but that individual results vary and cannot be predicted. She discusses common side effects including temporary pain and swelling at the injection site.
The patient asks clarifying questions. Dr. Martinez documents the informed consent discussion thoroughly, including the off-label status, mixed evidence, and realistic outcome expectations. Together, they decide to proceed with a trial of LP-PRP injections at a dose targeting the 5-10 billion platelet range supported by current evidence, with follow-up assessments at 3 and 6 months using standardized outcome measures.
This vignette illustrates several principles: transparent regulatory disclosure, balanced evidence presentation, shared decision-making, realistic expectation-setting, and documentation. These elements protect both the patient and the clinician.
Contraindications: when not to use PRP
In 2025, the International Research Group on Platelet Injections (GRIIP) published a formal consensus on indications and contraindications for PRP in patients with complex comorbidities. This is currently the most specific clinical guidance available for patient selection in complicated cases, validated by 31 international experts.
Absolute contraindications include active bacterial infection requiring antibiotic therapy, unstabilized hematologic malignancy, active solid cancer undergoing diagnosis or treatment, PRP injection near benign or malignant tumors or metaplasia, dental infection or recent invasive oral procedure, and local infection at the injection site.
Several conditions represent relative or conditional contraindications. Patients with HIV may proceed if they have an undetectable viral load and CD4 count above 350. Patients with hepatitis C should complete antiviral treatment before receiving PRP. Patients on chronic dialysis may proceed with monitoring but should avoid PRP on dialysis days. Patients with stable immunosuppression may proceed with careful infection surveillance.
Traditional contraindications also apply. These include platelet dysfunction syndrome, critical thrombocytopenia (platelet count below 50,000 per cubic millimeter), hemodynamic instability, and septicemia. Use of NSAIDs around the time of injection is a commonly cited relative contraindication, as NSAIDs may suppress the platelet activity that PRP depends on; specific cessation windows vary by protocol and practice. Corticosteroid injection at the treatment site within the prior month is also a relative contraindication.
Safety profile and adverse events
PRP carries a favorable safety profile relative to many musculoskeletal interventions, largely because it is autologous (derived from the patient’s own blood). However, it is not risk-free.
The most common side effects are injection site pain and tenderness lasting 2-5 days, temporary post-injection flare (increased pain and inflammation for 24-72 hours), swelling and bruising that resolves within 48-72 hours, and minor skin redness lasting 1-3 days. These are generally self-limiting and expected.
Rare but serious adverse events include infection (septic arthritis), estimated at approximately 0.035% for joint injections generally (about 3 per 7,900 procedures). A 2024 systematic review of 91 RCTs involving over 5,900 PRP knee injections found zero infections, suggesting the risk may be even lower for PRP when strict aseptic technique is followed. However, case reports of PRP-related infections do exist, and clinicians should not treat the risk as zero. Pseudoseptic reactions can mimic true infection with elevated white blood cell counts in the joint fluid and must be carefully differentiated. Nerve or tissue damage is rare and can be reduced with ultrasound guidance.
Special populations require additional consideration. Diabetic patients may experience more pronounced inflammatory reactions, and blood glucose monitoring may be advisable. Patients with prosthetic joints have limited safety data, and consultation with the orthopedic team is recommended.
Safety reporting
For suspected serious adverse events involving FDA-regulated medical products, devices, or drugs, clinicians can consider reporting via FDA MedWatch, consistent with institutional policy and applicable requirements.
What we do not know yet: evidence gaps
Transparency about what remains unknown builds trust with patients and reflects the honest state of the science. The following are the most significant evidence gaps in PRP for musculoskeletal medicine.
No standardized preparation protocols exist across the field. Different PRP systems produce different products with different platelet concentrations, leukocyte content, and activation methods. This makes comparing results across studies extremely difficult and is the single biggest contributor to conflicting findings.
Long-term data beyond 2 years is largely absent. Most studies follow patients for 6-12 months, with a smaller number reaching 24 months. We do not know whether PRP benefits persist, diminish, or require repeat treatment cycles over longer time horizons.
No formal society guidelines exist for PRP use in tendinopathy, ligament repair, or spinal applications. The guideline landscape is limited almost entirely to knee OA, leaving clinicians in other areas without formal recommendations.
Patient stratification remains a challenge. No validated biomarkers currently predict which patients will respond well to PRP and which will not. Recent dose-response data suggest that 5-10 billion platelets per injection may be a target range for knee OA, with doses below 2.5 billion appearing ineffective. However, the optimal dose for tendinopathy, plantar fasciitis, and other conditions remains unclear. Whether very high doses (over 10 billion) provide additional benefit, plateau, or potentially reduce outcomes is still being studied.
Cost-effectiveness data is limited. Few studies have conducted rigorous economic analyses comparing PRP to alternative treatments over meaningful time periods.
The AAOS established the Orthobiologics Registry (OBR) in May 2025, a pilot program at 10 sites specifically designed to generate the real-world evidence that is currently lacking. This registry aims to address preparation standardization, long-term outcomes, and patient selection questions.
What this means in practice: When patients ask whether PRP is “proven,” the honest answer is that the evidence is growing and encouraging for certain conditions, but important questions remain unanswered. Clinicians who offer PRP should frame it as an evolving field rather than an established standard of care for most indications.
Who may be a candidate for PRP
Based on the current evidence, the following clinical profiles appear most likely to benefit from PRP.
Patients with mild-to-moderate knee OA (KL grade I through III) who have not responded adequately to conservative measures such as physical therapy, weight management, and oral anti-inflammatories are the strongest candidates. Patients with lateral epicondylitis seeking longer-term relief beyond what corticosteroids provide also have good supporting evidence. Patients with plantar fasciitis resistant to conservative treatment have moderate supporting evidence. Athletes with hamstring injuries seeking faster return-to-play may see modest benefit.
Patients with severe OA (KL grade IV) generally show diminished response, though carefully selected patients who are not surgical candidates may still be considered per ESSKA guidance. Patients with chronic Achilles tendinopathy or those seeking ACL reconstruction augmentation currently have weaker or conflicting evidence. PRP is not a substitute for surgical intervention when surgery is clearly indicated.
Response rates vary. Not every patient will experience meaningful improvement, and individual outcomes cannot be predicted or guaranteed. Clinicians should set expectations using population-level data while emphasizing that individual response depends on many factors, including disease severity, preparation method, platelet dose, injection technique, and patient biology.
Frequently asked questions
Is PRP FDA-approved for joint injections?
No. PRP preparation devices are FDA-cleared under the 510(k) pathway for bone graft handling only. All injection applications for joints, tendons, and soft tissue are considered off-label. Off-label use is legal, but patients must be informed of this status.
How many PRP injections are typically needed?
Protocols vary. For knee OA, both the AAOS and ESSKA suggest 1-3 injections spaced weekly or biweekly. ESSKA allows up to 4 injections per cycle at 1-3 week intervals. The optimal number of injections has not been definitively established.
How long do PRP results last?
In studies of knee OA, benefits are most consistently observed at 6-12 months. Some patients report sustained improvement beyond 12 months, while others may need repeat injections. Long-term data beyond 2 years is limited.
Is PRP painful?
Most patients experience injection site pain and tenderness for 2-5 days after the procedure. A temporary flare of increased pain and swelling is common in the first 24-72 hours and is generally self-limiting. Serious complications are rare.
Does insurance cover PRP injections?
Most insurance plans do not cover PRP for musculoskeletal injections because these uses are off-label. Patients typically pay out of pocket. Costs vary by practice, region, and preparation system. Clinicians should discuss financial expectations with patients before treatment.
Which PRP preparation is best?
The best preparation depends on the tissue and the patient. For knee OA, evidence broadly favors LP-PRP, though the only direct head-to-head RCT comparing LP-PRP and LR-PRP found no significant difference at 12 months. For rotator cuff repair augmentation, LP-PRP shows more consistent benefit. For tendon conditions, evidence is mixed: LR-PRP has supporting data for lateral epicondylitis, while patellar and chronic Achilles tendinopathy show less consistent results regardless of preparation. Total platelet dose may matter as much as the LP versus LR label, with positive knee OA trials clustering around 5-10 billion platelets per injection. No single preparation has been proven definitively superior across all applications.
How many platelets does a PRP injection need to be effective?
There is no universally agreed-upon minimum platelet dose, and no professional society currently endorses a specific number. Recent evidence suggests that doses below approximately 2.5 billion platelets per injection are unlikely to produce clinical benefit for knee OA. Doses above 5 billion show consistent improvement in pain and function. Some research points to a possible “sweet spot” in the 5-10 billion range, with doses above 10 billion potentially showing diminishing returns. The frequently quoted “10 billion threshold” originates from a single 2021 RCT (Bansal et al.) and is not a settled standard. Clinicians should focus on absolute delivered platelet dose, not just concentration multiples over baseline.
Can PRP replace surgery?
PRP should not be presented as a replacement for surgery when surgical intervention is clearly indicated. Some patients may use PRP as part of a conservative management strategy before considering surgery, or as an adjunct to surgical procedures, but this decision should be individualized based on clinical assessment.
What conditions have the strongest PRP evidence?
The strongest evidence supports PRP for mild-to-moderate knee OA, lateral epicondylitis, and plantar fasciitis. Evidence is weaker or conflicting for Achilles tendinopathy, rotator cuff repair augmentation, and ACL reconstruction.
Should patients stop taking NSAIDs before PRP?
There is no universal consensus on the exact NSAID cessation window before PRP. NSAIDs may impair platelet function and are commonly held for at least 48 hours before the procedure in clinical practice, though some protocols recommend longer windows of 1-2 weeks. Neither the ESSKA ORBIT consensus nor the AAOS Technology Overview specifies an exact cessation timeframe, though both broadly support avoidance around the time of injection. Clinicians should consult their institutional protocols, and patients taking aspirin or other antiplatelet agents for cardiac indications should discuss any changes with their prescribing provider before stopping.
Key takeaways
- PRP devices are FDA-cleared for bone graft handling only. All musculoskeletal injection applications are off-label and require informed consent disclosure.
- The strongest evidence supports PRP for mild-to-moderate knee OA (KL I-III), lateral epicondylitis, and plantar fasciitis, with benefits most consistently observed at 6-12 months.
- Professional societies disagree: ESSKA supports PRP for knee OA (Grade A), ACR/AF conditionally recommends against it for knee OA, and AAOS makes no recommendation either way.
- The leukocyte concern in PRP is mainly about neutrophils, while monocytes and lymphocytes appear net beneficial. Centrifugation typically reduces neutrophils and increases lymphocytes, even in “leukocyte-rich” preparations.
- Platelet dose matters: positive knee OA trials cluster around 5-10 billion platelets per injection, while doses below 2.5 billion show consistent failure. The “10 billion threshold” claim derives from a single 2021 RCT, not a settled standard.
- Preparation variability (LP-PRP versus LR-PRP, different platelet doses, different activation methods) is the primary driver of conflicting research findings.
- Individual results vary and cannot be guaranteed. Approximately 60-70% of knee OA patients in large cohorts report meaningful improvement, but 30-40% may not respond.
- Absolute contraindications include active infection, unstabilized hematologic malignancy, and active cancer undergoing treatment.
- Clinicians considering adding PRP to their practice should seek hands-on musculoskeletal orthobiologic training to ensure proper technique, patient selection, and documentation practices.
Adding PRP to your practice
PRP is a technique where the literature alone cannot teach you what you need to know. Preparation system selection, dosing calibration, neutrophil-aware processing, ultrasound-guided injection technique, and informed consent documentation all require practical skill that develops through supervised, hands-on instruction. The clinicians most likely to deliver consistent results are those who pair their reading of the evidence with structured training in technique and patient selection. RMA’s regenerative medicine training courses are designed for licensed clinicians who want to translate the evidence reviewed in this article into reproducible bedside practice.
About Regenerative Medicine Academy
Regenerative Medicine Academy (RMA) is a medical education company providing hands-on, small-group regenerative medicine training courses for licensed healthcare professionals. RMA does not provide clinical treatments or medical services. All course content is educational and designed to support clinicians in making informed, evidence-based decisions within their scope of practice. For more information about upcoming training dates and online regenerative medicine education, visit regenmedacademy.com.
Off-label use note
The procedures discussed in this article may involve off-label use of FDA-cleared devices. Off-label use means the FDA has not specifically approved the device for the described indication. Clinicians may use FDA-cleared devices off-label in their clinical judgment, but must obtain informed consent, discuss evidence, risks, and alternatives, and document thoroughly.
Platform/jurisdiction note
Scope of practice, supervision requirements, and corporate practice of medicine rules vary by state. Clinicians should consult their state medical board, malpractice carrier, and legal counsel regarding compliance in their jurisdiction before offering regenerative procedures.