When platelet-rich plasma (PRP) injections produce different outcomes from one clinic to the next, the answer is rarely the biology. It is usually the way the procedure is prepared, targeted, and supported. This guide walks through five preventable errors that quietly undermine PRP results in everyday practice, and explains how structured training closes each gap.
TLDR: Platelet-rich plasma outcomes depend heavily on dose, delivery technique, patient selection, peri-procedural medication management, and preparation choices. Published evidence points to five recurring mistakes that reduce clinical benefit: sub-therapeutic dosing, landmark-only injections, poor candidate screening, NSAID mismanagement, and inconsistent preparation, including the use of pre-activation that is generally not recommended for musculoskeletal applications. PRP devices are FDA 510(k)-cleared for bone graft handling, so most clinical injection use is off-label. Structured training, ultrasound skills, standardized workflows, and clear informed consent give clinicians more reproducible results. Evidence remains mixed, and outcomes vary in every patient.
Important Disclaimer
Regenerative Medicine Academy (RMA) is an education company providing training for licensed clinicians. This article is educational content and does not constitute medical advice, legal counsel, or any guarantee of clinical outcomes. Techniques discussed may be used off-label and are subject to state and federal regulations. Clinicians are responsible for understanding FDA status, scope of practice, informed consent, and malpractice implications before using any technique in practice. Individual clinical judgment and patient-specific factors must guide all clinical decisions.
PRP has been studied for more than two decades. Yet two clinicians using the same kit, the same patient profile, and the same target joint often see very different outcomes. One patient feels real relief. Another feels nothing. After enough mixed results, some clinicians quietly begin to doubt the therapy itself.
The published evidence tells a different story. When researchers compare PRP trials head to head, most of the variation comes from things clinicians control: how the product is prepared, how it is delivered, who receives it, and what happens before and after the injection. Those variables are teachable. They are also where most preventable mistakes happen.
This guide walks through the five most common PRP mistakes and what proper training changes about each one. The goal is fewer surprises for patients, stronger outcomes for your practice, and clearer informed consent for everyone involved.
Why PRP outcomes vary so widely between clinics
PRP outcomes vary because PRP is not one product. It is a family of autologous (patient-derived) blood preparations that differ in platelet dose, white blood cell content, activation method, and injection technique. When any of those variables drift, so do results.
A widely cited review of commercial PRP systems found that final platelet concentration can range from about half of baseline whole blood to nearly ten times baseline, depending on the device and draw volume. Similar variability shows up in white blood cell content, injection volume, and growth factor profile. Two clinics both using “PRP” can deliver very different biologics.
On top of product variability, injection accuracy, patient selection, and NSAID use all shape the healing environment. Most of these are training problems, not biology problems. The good news: each one can be systematically improved with education, workflow redesign, and supervised practice.
What this means in practice: if your PRP outcomes feel unpredictable, the fix is almost never a new kit. It is a tighter workflow across dose, delivery, patient selection, and peri-procedural care.
How PRP is supposed to work, briefly
PRP concentrates platelets from a patient’s own blood. Platelets contain small storage sacs called alpha granules, which release proteins called growth factors. These include platelet-derived growth factor (PDGF), transforming growth factor-beta (TGF-beta), vascular endothelial growth factor (VEGF), and insulin-like growth factor (IGF-1).
When delivered into a joint, tendon, scalp, or skin, those growth factors signal nearby cells to multiply, make new collagen, form new blood vessels, and modulate inflammation. Researchers are studying whether this cascade supports tissue repair and symptom relief in specific clinical scenarios.
Research also suggests a dose-response relationship in many indications. Higher platelet doses tend to produce stronger biological signals, though clinical benefit still depends on many other factors. That is why under-dosing matters, and why the first mistake on this list is about dose.
The regulatory context every PRP clinician should know
PRP preparation systems are cleared under the FDA 510(k) pathway as Class II medical devices for intraoperative use with bone graft material. That clearance covers how the device processes blood to improve bone graft handling. It does not approve PRP for any specific injection use in patients.
This means almost every common clinical use of PRP, including knee osteoarthritis (OA), tendinopathy, hair loss, aesthetic applications, and sexual health indications, is considered off-label. Off-label use is legal when it reflects sound clinical judgment. But marketing language cannot state or imply FDA approval for these uses.
Clinicians should document off-label status clearly in informed consent, avoid cure or guarantee claims, and frame outcomes in terms of possible symptom support and individual variability. Many of the hardest regulatory mistakes clinicians make are not technique errors. They are marketing and consent errors. Good training covers both.
Mistake 1: Under-dosing with sub-therapeutic PRP
The most common PRP mistake is not a technique error. It is giving too little PRP to produce a meaningful biological signal. Researchers have repeatedly shown that final platelet dose, not simply the presence of PRP, drives clinical response.
Published literature often describes a “therapeutic” PRP as a product that concentrates platelets to roughly three to five times baseline whole blood levels. Commercial kits vary widely. A well-known review of commercial systems showed concentration fold-increases ranging from about 0.5x to nearly 10x across marketed devices. Two “PRP” injections can therefore deliver very different actual doses. A 2025 meta-analysis in the American Journal of Sports Medicine found that higher platelet concentrations correlated with greater symptom and function benefit in knee osteoarthritis, supporting a threshold-effect framework rather than a one-size-fits-all target.
One high-profile negative trial for knee OA, the 2021 RESTORE study published in JAMA, found that PRP was no better than saline at 12 months. RESTORE used a leukocyte-poor preparation; some reviewers have argued that the platelet dose was lower than what positive trials have used, which is one of several possible explanations for the negative result. Studies using larger draws and higher concentrations have reported more favorable symptom and function outcomes, though heterogeneity remains high and individual response varies.
Dose also shifts patient by patient. A 2023 analysis in Arthroscopy showed that final PRP platelet count varies directly with a patient’s baseline blood platelet count, age, sex, and body mass index. The same kit run on two different patients can produce two different doses.
What this means in practice: clinicians should think in terms of total platelets delivered (volume multiplied by concentration), not a kit name. Training should cover how to interpret a baseline complete blood count (CBC), adjust draw size within safe limits, select spin protocols thoughtfully, and verify yields where possible. That is the difference between running a kit and managing a process.
Mistake 2: Landmark-only (blind) injections without imaging guidance
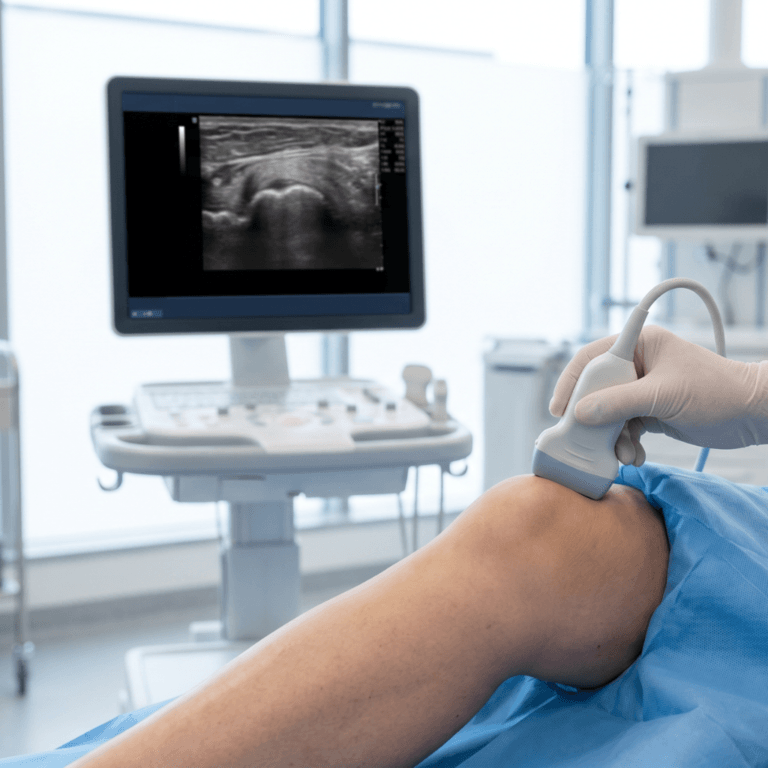
The second common mistake is relying on surface anatomy alone when imaging would place the needle more accurately. Multiple systematic reviews indexed on PubMed show that ultrasound-guided musculoskeletal injections are consistently more accurate than landmark-only techniques. Accuracy matters because PRP only works if it reaches the intended tissue.
A 2021 systematic review of Level I randomized controlled trials covering knee injections found that ultrasound guidance improved accuracy at every anatomical portal when compared with blind injection. A broader 2024 umbrella review across multiple joints reached a similar conclusion, with the largest accuracy advantage in the shoulder. For small joints and peritendinous targets, the accuracy gap is often larger still.
Blind intra-articular knee injection accuracy is commonly reported near 70 percent, while ultrasound-guided injection accuracy rises to somewhere between 87 and 100 percent depending on joint and portal. For shoulders and other technically demanding targets, palpation-based accuracy can drop well below 95 percent, while ultrasound routinely exceeds that threshold.
For tendinopathies, accuracy is only part of the story. Peritendinous placement, in-tendon fenestration, and targeting specific pathologic regions (for example the common extensor origin in lateral epicondylitis) all benefit from real-time imaging. Blind injection cannot reliably deliver those techniques.
What this means in practice: clinicians who inject PRP should become comfortable using diagnostic ultrasound for the targets they treat most often. That skill set includes scanning, needle tracking (in-plane and out-of-plane), and matching approach to pathology. Training should include supervised, hands-on ultrasound practice, not just didactic instruction.
Mistake 3: Poor patient selection and missed contraindications
The third mistake is offering PRP to patients who should not receive it. Poor candidate selection undermines outcomes, increases risk, and creates informed consent problems. PRP has absolute and relative contraindications that clinicians should screen for systematically.
Before discussing candidate criteria, a few terms are worth defining. Platelet disorders are conditions where platelets are too few or do not work properly. Anticoagulants are medications that reduce blood clotting. Autoimmune flares are periods when the immune system is especially active against the body’s own tissues.
Published reviews describe both absolute and relative contraindications. Absolute contraindications include platelet disorders that prevent meaningful yield, active local or systemic infection, and certain active malignancies. Relative contraindications include significant thrombocytopenia, ongoing anticoagulant therapy, advanced liver disease, uncontrolled diabetes, and active autoimmune flares. For cosmetic PRP, active skin conditions at the planned injection site raise the risk of poor cosmetic outcomes.
The table below summarizes commonly cited contraindications and the reasoning behind them.
| Category | Example contraindications | Clinical reasoning |
| Hematologic | Thrombocytopenia, platelet dysfunction, active anticoagulation, hemophilia | Inadequate platelet yield and bleeding risk |
| Oncologic | Active malignancy, especially hematopoietic cancer | Theoretical concern about growth factor signaling; case-by-case review for history |
| Infectious | Local or systemic infection at time of injection | Risk of seeding or spreading infection |
| Hepatic and metabolic | Advanced liver disease, uncontrolled diabetes | Impaired clotting and healing |
| Autoimmune | Active lupus, rheumatoid flare, multiple sclerosis relapse | Unpredictable inflammatory response |
| Obstetric | Pregnancy and lactation | Limited safety data |
| Dermatologic (cosmetic PRP) | Active acne, eczema, rosacea, keloid tendency | Cosmetic outcome and flare risk |
What this means in practice: a checklist-driven intake process that includes a CBC review, medication reconciliation, oncology screening, and site examination catches most problems before the needle is ever drawn. Training should cover structured intake templates, documentation habits, and informed consent language that clearly states off-label status and patient-specific risks.
Mistake 4: NSAID mismanagement before and after PRP
The fourth common mistake is ignoring non-steroidal anti-inflammatory drugs (NSAIDs) around the time of a PRP injection. NSAIDs reduce platelet function and modulate the inflammatory cascade PRP is thought to activate. Allowing patients to continue them through key windows can blunt the response.
A 2022 systematic review in Orthopaedic Journal of Sports Medicine concluded that aspirin, acetaminophen, and nonselective NSAIDs should be considered for pre-procedural suspension because they reduce platelet function and growth factor release. An in vitro study of patients taking twice-daily ibuprofen or diclofenac showed measurable reductions in platelet aggregation in PRP prepared from their blood. Aspirin’s effect lasts the full platelet lifespan, roughly seven to ten days.
After the injection, most published protocols recommend avoiding NSAIDs for a period of weeks. The idea is that PRP relies on an orchestrated inflammatory response to initiate healing. A systematic review of post-injection rehabilitation protocols reported that most restrict NSAIDs after PRP, commonly for more than two weeks.
The table below summarizes commonly cited pre- and post-injection medication considerations from the published literature. These are ranges drawn from the literature, not a prescription. Clinicians should tailor decisions based on cardiovascular risk, bleeding risk, and shared decision-making.
| Medication | Commonly cited pre-PRP hold | Commonly cited post-PRP hold |
| Aspirin | 7 to 10 days | 2 weeks or more |
| Ibuprofen, diclofenac | 3 to 7 days | 2 to 6 weeks |
| Naproxen | 24 to 48 hours at minimum, often up to 7 days | 2 to 6 weeks |
| Acetaminophen | Consider individualized hold | Often preferred analgesic |
| Local corticosteroid injection at same site | 4 to 6 weeks before PRP | Case-by-case |
What this means in practice: a pre-procedure medication checklist and a standardized post-procedure discharge handout prevent most NSAID-related problems. Training should cover patient education scripts, how to weigh anticoagulant indications against PRP timing, and how to document shared decisions in the chart.
Mistake 5: Inconsistent preparation, the leukocyte debate, and unnecessary activation
The fifth mistake is treating all PRP as the same PRP, and applying assumptions that the published literature does not actually support. Preparation method, leukocyte content, and activation approach all shape the final biologic. Choosing them by convenience, or by tradition that the data does not back up, undermines outcomes and obscures lessons across cases.
Preparation variability is well documented. Across commercial systems, final platelet concentration ranges from roughly 0.5x to 10x baseline, with very different volumes and white blood cell profiles. Even the same kit can yield different products depending on operator technique and baseline patient values. The right framework is not “what kit do I use” but “what total platelet dose does my workflow reliably deliver, and what is actually in my final product.”
The leukocyte question: an unsettled debate built on incomplete data
The choice between leukocyte-rich PRP (LR-PRP, which retains higher white blood cell levels) and leukocyte-poor PRP (LP-PRP, which is filtered to minimize them) is one of the most discussed topics in PRP preparation. It is also one of the most poorly resolved, and not because the underlying biology is uninteresting. The honest assessment is that many of the published comparisons rest on inconsistent measurement and reporting, which makes “which is better” a question that often cannot be answered cleanly from the data we have.
A more useful starting point is a set of questions to ask of any study comparing LR-PRP and LP-PRP. These questions are how a careful clinician should read the literature, and they double as a checklist for evaluating any future device claim or comparative trial.
The first question: what was the actual measured leukocyte concentration in the product used? Many published studies label preparations as “leukocyte-rich” or “leukocyte-poor” based on the kit type, the spin protocol, or the manufacturer’s claim, without quantifying the actual leukocyte content at the time of preparation. When a study does not report measured leukocyte values, you do not actually know what was injected, and you should hold conclusions from that study loosely.
The second question: what was the patient’s baseline white blood cell count? Final leukocyte content depends on starting blood values, just as platelet content does. A so-called leukocyte-rich preparation made from a patient with a low baseline white blood cell count could deliver fewer total leukocytes than a so-called leukocyte-poor preparation made from a patient with a high baseline. Without knowing the baseline, you cannot interpret the final number.
The third question: what was the relative composition of those leukocytes? Neutrophils, lymphocytes, and monocytes have different signaling roles. A preparation dominated by neutrophils may behave biologically differently than one dominated by lymphocytes, even at the same total leukocyte count. Most published studies do not break down the leukocyte composition, which is another piece of information missing from the comparison.
The fourth question: were leukocyte content and platelet dose reported together? Leukocyte content and platelet dose are typically correlated based on preparation method, but the correlation is not perfect. A study that reports only one of these variables provides only half the information needed to interpret the result.
When the literature is read with these questions in mind, the LR-versus-LP debate looks humbler than the often-quoted “LR for tendons, LP for joints” framing suggests. A 2022 in vitro study in Orthopaedic Journal of Sports Medicine showed that LR-PRP produced higher levels of certain growth factors and greater tenocyte (tendon cell) proliferation in rotator cuff cell culture. That is part of the basic science argument for LR-PRP in tendinopathy. But basic science is not the same as clinical evidence, and clinical comparisons in humans are inconsistent. A 2024 systematic review on knee OA found no consistent clinical superiority of one over the other in randomized trials, though the same review noted that leukocyte content was inconsistently reported across the included studies. The 2024 ESSKA-ORBIT consensus considers both LR-PRP and LP-PRP valid options for knee OA, with the explicit caveat that effectiveness is likely multifactorial and the dependence on leukocyte presence alone may be overestimated.
What this means in practice: clinicians should not treat the LR-versus-LP framework as settled. The conservative working defaults remain LP-PRP for intra-articular joint use and LR-PRP for some tendinopathies, but those are starting points based on basic science and theoretical concern, not on definitive clinical evidence. Until studies consistently report actual measured leukocyte content alongside platelet dose, any conclusion about superiority should be held loosely, and any device claim about leukocyte content should be evaluated against measured values rather than label language.
Activation: usually unnecessary and generally not recommended
Some preparation protocols include activating PRP before injection using exogenous agents such as calcium chloride, thrombin, or collagen. The original idea was that activation triggers platelet degranulation and growth factor release, ensuring the bioactive cargo is available immediately upon delivery.
Pre-activation is generally not recommended for musculoskeletal PRP injections. The reason is mechanical and straightforward. When PRP is activated upstream of the injection, growth factors begin to release during preparation and during the journey through the syringe and needle, before the product reaches the target tissue. By the time the activated PRP arrives at the joint, tendon, or other target, much of the bioactive signal has already been spent.
PRP activates naturally in vivo when it contacts tissue collagen, exposed extracellular matrix, and the body’s own clotting signals. Allowing this in situ activation lets growth factors release in the right place at the right time, where they can act on the cells you are trying to influence. The published comparative evidence between activated and unactivated PRP for musculoskeletal applications is limited, and there is no clear consensus that adding exogenous activation improves outcomes. Most well-designed musculoskeletal protocols default to unactivated PRP.
What this means in practice: clinicians should not pre-activate PRP for musculoskeletal injections without a specific evidence-based reason to do so. The default should be unactivated PRP, allowed to activate in situ at the target tissue. Time spent worrying about which activation method to use is generally time better spent ensuring an adequate platelet dose, accurate delivery, and appropriate patient selection.
A composite clinical vignette: when small errors compound
The following is a fictional composite based on patterns described in the published literature. It does not describe a real patient.
A 58-year-old recreational hiker presents to a private practice with six months of medial knee pain. Imaging confirms mild-to-moderate knee OA. The clinician recommends PRP. The patient continues twice-daily ibuprofen up to the morning of the injection. A small blood draw runs through a single-spin kit that concentrates platelets to about 2x baseline. The injection is landmark-guided with an anterolateral approach. The patient is told to resume ibuprofen within two days.
Four weeks later the patient reports no meaningful change.
On review, several common mistakes stack up. The delivered dose was likely below therapeutic targets reported in the literature. The ibuprofen almost certainly blunted platelet function and the post-procedure inflammatory response. The blind injection may not have reliably reached the intra-articular space. The patient was never screened with a CBC to help calibrate dose. No preparation rationale was documented, and no actual leukocyte or platelet count was verified.
A restructured workflow addresses each gap: pre-procedure NSAID guidance, CBC-informed dose planning, ultrasound guidance, an unactivated leukocyte-poor preparation appropriate to an intra-articular target, and a post-procedure plan that protects the healing window. The biology did not fail. The workflow did.
How structured training closes the gap
Training is the common denominator across all five mistakes. Strong training programs move clinicians from running a kit to managing a process that includes intake screening, imaging, dose planning, delivery, peri-procedural education, and outcome tracking.
Hands-on ultrasound practice under supervision builds the accuracy needed for real-world targets. Live-patient exposure with faculty feedback develops the judgment that videos and lectures cannot. A structured curriculum around contraindications, informed consent, off-label framing, and the standardization problem in the published literature helps clinicians communicate clearly with patients and document responsibly.
For clinicians building or refining their skills, hands-on musculoskeletal regenerative medicine training provides the live-patient experience and structured feedback needed to translate evidence into reproducible practice. Didactic foundations, which are also essential, can be covered in regenerative medicine e-learning courses that complement in-person training. Clinicians working in aesthetic applications may also find value in cosmetic regenerative medicine training, where similar principles of dose, patient selection, and technique apply to different tissues. Broader profession-level commitment to gathering real-world data is also reflected in the AAOS Orthobiologics Registry, announced in December 2025, which is designed to track standardized composition data alongside patient outcomes at scale.
Frequently asked questions from clinicians
Is PRP FDA-approved for knee osteoarthritis, tendinopathy, or hair loss?
No. PRP preparation devices are FDA 510(k)-cleared for bone graft handling. Clinical injection uses for knee OA, tendinopathy, hair loss, and similar indications are considered off-label. Clinicians should document off-label status in informed consent and avoid language suggesting FDA approval for these uses.
How should I counsel a patient whose prior PRP injection did not work?
Start by reviewing the prior workflow. Ask about the kit, dose, imaging guidance, medication use around the injection, and post-procedure instructions. Many disappointing PRP results reflect one or more of the mistakes described above. A candid conversation about what is known, what is uncertain, and what individual response factors look like helps patients make an informed decision about a second attempt.
Does ultrasound guidance really change outcomes, or only accuracy?
Systematic reviews most consistently show improved accuracy. Accuracy is a plausible driver of clinical outcome, since the biologic can only act where it lands. Some outcome studies favor guided injections, especially for small joints and tendons. Direct outcome-level comparisons vary by indication, so clinicians should present findings with appropriate nuance.
What baseline labs or screening steps are commonly recommended before PRP?
Published reviews commonly recommend a CBC, a review of medications including anticoagulants and NSAIDs, a focused history on oncology and autoimmune disease, and examination for local infection at the planned injection site. Clinicians should match their intake to their patient population and local standards.
Is LR-PRP or LP-PRP better?
That question is harder to answer than it sounds, and “which is better” may be the wrong starting point. A more useful first question is whether any given study comparing the two actually measured and reported the leukocyte content of the products used. Many published comparisons label preparations as “leukocyte-rich” or “leukocyte-poor” based on the kit or protocol, without quantifying actual leukocyte counts at the time of preparation. When measurement is missing, the comparison provides limited evidence regardless of the result. The conservative working defaults remain LP-PRP for intra-articular joint use and LR-PRP for some tendinopathies, but those are starting points based on basic science and theoretical concern, not on definitive clinical evidence.
Should I activate PRP before injection?
Pre-activation is generally not recommended for musculoskeletal PRP. PRP activates naturally in vivo when it contacts tissue collagen and the body’s own clotting signals, and pre-activation with exogenous agents can release growth factors during preparation and delivery, before the product reaches the target tissue. The published comparative evidence between activated and unactivated PRP is limited, and most well-designed musculoskeletal protocols use unactivated PRP.
How much training is reasonable before offering PRP?
There is no single answer. Clinicians new to orthobiologic injections generally benefit from didactic foundations, hands-on ultrasound training, supervised procedural practice, and a period of case review. Scope of practice, state regulations, malpractice coverage, and institutional policy all play a role. Clinicians should consult legal counsel and their malpractice carrier when expanding procedural offerings.
What should a patient expect after a PRP injection?
Most patients experience a local soreness or flare for one to three days after the injection, followed by a gradual response over weeks. Results vary widely by indication, patient factors, and preparation. Clinicians should set realistic expectations in advance, schedule a follow-up, and use a validated outcome measure where possible.
Key takeaways
- Most preventable PRP failures trace back to five recurring mistakes: under-dosing, blind injection, poor patient selection, NSAID mismanagement, and inconsistent preparation.
- Dose matters. Clinicians should think in total platelets delivered, and adjust to the patient rather than simply running a kit.
- Ultrasound guidance improves accuracy across most musculoskeletal targets, especially small joints and tendons.
- A checklist-driven intake process catches most contraindications before the injection.
- NSAID timing around PRP should be guided by published literature, balanced with each patient’s cardiovascular and bleeding risk.
- Leukocyte-rich versus leukocyte-poor PRP remains an unsettled debate. Many studies that compare the two do not measure or report actual leukocyte content, which limits how confidently any conclusion can be drawn.
- Pre-activation of PRP with exogenous agents such as calcium chloride or thrombin is generally not recommended for musculoskeletal injections. PRP activates naturally in vivo when it contacts tissue collagen, and pre-activation can release growth factors before they reach the target tissue.
- All of these are training issues. Structured education, hands-on imaging practice, and live-patient experience close each gap.
RMA Disclosure
Regenerative Medicine Academy (RMA) is an education company that provides clinician training in some of the techniques discussed in this article. This content is educational and does not constitute a claim of clinical superiority, a guarantee of outcomes, or a substitute for individual clinical judgment.
Off-label use note
Procedures discussed in this article involve off-label use of FDA-cleared devices. PRP preparation devices are cleared through the FDA’s 510(k) pathway for producing platelet-rich preparations to mix with bone graft materials in orthopedic surgical procedures. All intra-articular, peritendinous, and other musculoskeletal injection applications are off-label. Clinicians may use FDA-cleared devices off-label based on clinical judgment but must obtain informed consent, discuss evidence, risks, and alternatives, and document thoroughly.
Platform and jurisdiction note
Scope of practice, supervision requirements, and corporate practice of medicine rules vary by state. Clinicians should consult their state medical board, malpractice carrier, and legal counsel regarding compliance in their jurisdiction before offering regenerative procedures.
For clinicians ready to strengthen their procedural skills
Clinicians ready to refine their workflows and build defensible documentation around PRP and related orthobiologic techniques can explore RMA’s full course catalog. The catalog covers musculoskeletal, cosmetic, sexual health, and adipose tissue applications, with small-group hands-on training, private one-on-one options, and on-site delivery for practices that want their team trained together with their own patients and workflow.